Liver Disease
LIVER DISEASE
Normal Liver:
The liver is the largest solid organ in human body. It weighs about 1600 Gm in men and 1400 gm in women. It is a triangular or pyramid in shape and lies sideways in the upper right half of the abdomen with the base of the pyramid on the right side and the tip at the middle of the upper abdomen. Most of the liver is under the lower ribs and under normal conditions may not be felt by pressing on the abdomen except for its left portion that may be felt in the upper mid abdomen.
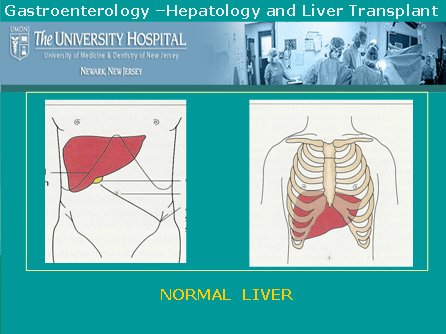
The gall bladder that stores bile, lies on its undersurface. The normal liver is brown in color, its surface is smooth band it is soft and pliable in texture.
Under
Microscope:
The
liver has well organized layers or plates of cells called liver cells.
The cell plates are supported in a matrix of small amount of fibrillar
scaffolding called connective tissue. The connective tissue usually
accounts for 5-10% of normal liver weight. In addition the liver has
smaller branches of blood vessels that supply and drain blood into and
out of liver. It also has fine nerves and lymphatics.
As
shown below liver cells are arranged as plates or cords of cells with
collection of vessels at the center and at outer rim of the radiating
liver cell cords.

Figure of normal liver as seen under microscope.
What does a normal Liver Do?:
- Acts as a filter for toxic substances and metabolizes various drugs and helps its elimination from the body.
- Makes various proteins, essential vitamins, hormones and chemicals for normal body function
- Makes bile and pours it out into the gall bladder that helps digestion
- Facilitates large number of metabolic processes of the body. It plays key role in the metabolism of carbohydrates, fat, and proteins.
- Makes various substances/factors that prevent excessive bleeding
Tests
for Liver Disease:
Different
tests are done to detect presence of liver disease. These tests can
be put in three distinct categories:
- Tests to assess normal function of liver, also called Liver Function Tests or liver chemistry
- Tests
that detect complications of liver disease that occurs as the liver
disease progresses and becomes established and chronic.
- Tests
specific for certain diseases and biopsy of liver.
Liver Function Tests:
These tests are based on normal functioning of liver. These tests essentially look for concentrations of certain elements or enzymes in the blood that are otherwise maintained within a tight range of normal values. When the liver does not function normally because of injury and disease the blood concentrations of theser substances deviate from their normal range. Most of the time these tests do not indicate the actual cause of the liver injury or disease, they only suggest that the liver is not functioning to its full normal capacity and is injured or is diseased. Identifying the cause of liver damage will probably require more definitive and specific tests.
Commonly used tests for liver function include the measurements of the following in the blood:
| Tests |
Normal |
If
abnormal then indicates |
| Total Bilirubin |
0.2-1.0
mg% |
Indicates
Jaundice and severity of liver damage |
| Transaminase /
Aminotransferase |
|
| ALT |
5-35 IU/L |
Indicates liver
cell injury |
| AST |
5-40 IU/L |
Indicates
Liver cell injury |
| Alkaline Phosphatase |
35-130 IU/L |
Indicates
poor ability to secrete bile and other Selective dysfunction |
| Albumin |
3.5-5.0 Gm% |
Chronic
liver disease |
| Prothombine
time/INR |
12-15 sec/1.01 |
acute liver
injury |
Tests
that detect complications of liver disease that sets-in as the liver disease
progresses and becomes established and chronic:
These
tests usually are complimentary to assess the gross appearance /distortion
of liver, and presence of complications of liver disease. Examples are
looking for nodular irregular liver, altered texture of the liver, abnormal
varicose veins inside abdomen, collection of fluid in side the abdomen,
enlargement of spleen and presence of liver tumor or cancer etc.
These
tests are:
- Ultra
sound imaging of liver
- CT
scan of liver and abdomen
- MRI
of Liver and abdomen
Tests
specific for certain diseases and biopsy of liver:
There
are specific tests to identify the cause of underlying liver disease.
A thorough medical history, clinical examination of the patients give
a clue to possible causev of the liver disease and then those tests
are carried out to identify the causative agent.
Following
are some of the specific tests foe the causes of liver diseases:
- Blood
tests for Viral hepatitis A, B, C, Delta, E and other less common
viral hepatitis.
- Hemochromatosis:
A disease with abnormal storage of iron in liver and body
- Wilson's
Disease: A disease characterized by accumulation of copper in liver
- Primary
Biliary Cirrhosis (PBC)
- Primary
Sclerosing Cholangitis (PSDC)
- Autoimmune
hepatitis
- Other
rare metabolic diseases of liver
- Liver
Cancer: Screening test for alfa feto protein and imaging.
Liver
Biopsy:
The process involves removing a tiny piece of liver by specialized needle and examining the tissue sample after proper processing and staining under a microscope. Patients are carefully selected to avoid and minimize risk of bleeding from the biopsy site. Biopsy is done either by approaching the liver in-between the ribs or through a vein in the neck and advancing a thin tubing (catheter guided biopsy needle) into the liver.
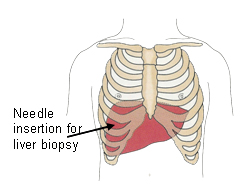

Figures: Liver Biopsy
Common
Causes of Liver Disease:
Liver
injury and liver disease can occur from a variety of causes. Various
agents and disease conditions that commonly cause liver damage are the
following:
- Viral
infection (hepatitis A, B, C, Delta and E virus infections)
- Alcohol
- Obesity
- Complication
of certain medications
- Abnormalities
of hepatic veins: Budd-Chiary syndrome
- Exposure
to chemicals
- Metabolic
and genetic disorders
- Cancer
Symptoms and signs of Liver Disease:
Some of the signs and symptoms of liver disease include:
- Jaundice(Yellowing Of The Skin And Eye)
- Pruritus(Itching)
- Dark Or Tea-Colored Urine
- Muscle Wasting
- Skin may show "liver spots" , palm may be unduly bright mottled red
- Retention Of Fluid: This May Take The Form Of Ascites (Swelling Of The Abdomen With Fluid) And Or Swelling Of Ankles Or Legs With Fluid.
- Easy Bruising And Bleeding (Bleeding Gums Or Frequent Nosebleeds)
- Vomiting Blood
- Blood In The Stool (Bright Red Blood Or Black, Tar-Like Stool)
- Mental Confusion (Encephalopathy), sleep disturbance
- General feeling of ill-health: These are general symptoms not necessarily indicative of liver disease but reflect constitutional symptoms of poor health and illness in-general. These are fatigue, weight loss, debility, weakness, malaise, and poor appetite.
- In women: Menstural irregularity, infirtilty and early menopause are not uncommon with advanced liver disease.
- In men: decreased libido, erectile dysfunction, impotence, sterility, thinning of body hair and prominence of breast are seen with advanced liver disease.
Not every person with liver disease has all the above symptoms and signs. Manifestations of symptoms and signs are very variable. T one end of the wide spectrum of the disease an individual may not have any symptom despite the presence of established chronic liver disease and the diagnosis may be made following detection of abnormal blood tests at general health examination. On the other extreme a person may have most of the features described above and may be quite debilitated.
Liver Diseases and Conditions:
I.
Cirrhosis
Continued
or chronic injury to liver damages the liver cells. The damaged liver
cells are replaced by scar tissue. Over time, the build-up of scar tissue
becomes so great that it impacts blood flow through the liver, destroying
more liver cells and ultimately leading to greater and greater loss
of liver function � a condition called cirrhosis.
Causes
of Cirrhosis:
Alcohol
remains the most common cause of cirrhosis of liver. Other causes
include chronic hepatitis C virus and hepatitis B virus infection,
autoimmune liver diseases (autoimmune hepatitis, Primary biliary cirrhosis,
primary sclerosing cholangitis), abnormal deposition of iron (Hemochromatosis),
or copper (Wilson's Disease), exposure to drugs and toxins and other
genetically inherited diseases like Cystic fibrosis and Alfa 1-antitrypsin
Deficiency.
Symptoms
and Signs of Cirrhosis:
As
cirrhosis evolves patients develop various signs and symptoms of liver
disease namely jaundice (yellowing of the skin and eye), pruritus
(itching), dark, tea-colored urine, weight loss, muscle wasting, fatigue,
ascites (swelling of the abdomen with fluid), easy bruising and bleeding
(bleeding gums or frequent nosebleeds), vomiting blood, blood in the
stool (bright red blood or black, tar-like stool), and mental confusion
(encephalopathy). Cirrhosis of any cause increases the risk of developing
liver cancer.
Not
all these features may be present at any given time but may evolve
as the disease progresses.
Diagnosis:
Presence
of features mentioned above helps physicians to strongly suspect the
diagnosis of cirrhosis. This can be further supported by blood tests,
imaging the liver by ultrasound or CT scan and in instances by a liver
biopsy. Liver biopsy is a test where a thin core of liver tissue is
removed from the liver by inserting a thin needle into the liver after
anesthetizing the skin of the right-lower chest. The tissue sample
is examined under microscope.
II.
Hepatitis:
Inflammation
of liver is called hepatitis. The liver can get inflamed (sore) by a
number of injurious things like: viruses (viral hepatitis), alcohol
(alcoholic hepatitis), too much of fat accumulation in liver (non alcoholic
steato hepatitis or NASH), deranged immune mechanism (autoimmune hepatitis),
drugs, chemicals and toxins (toxic hepatitis) etc.
Different
types of Hepatitis:
1.
Viral hepatitis:
Commonly
seen viruses that infect the liver causing hepatitis are named as
Hepatitis virus A, Hepatitis virus B, and Hepatitis virus C. Other
viruses that can cause hepatitis include hepatitis virus D, hepatitis
virus E, hepatitis virus G, infectious mono virus and CMV.
Viral
hepatitis is a major public health issue and remains the most common
cause of liver disease world wide. In the USA over 300,000 get acute
hepatitis due to one or the other viral infections. Over 15,000 Americans
die each year from complications of chronic viral hepatitis and is
estimated that in the next two decades annual death rate from all
viral hepatitis together will be around 25,000.
Different
types of viral hepatitis are given below:
i.
Hepatitis A:
This
used to be called infectious hepatitis. Infection occurs through
contaminated food or water. Contaminated water, ice, uncooked contaminated
food, uncooked shellfish (oysters, clams, mussels) are not an uncommon
source of infection. It is estimated that annually around 75,000
cases of acute hepatitis A occur in USA .
Persons
at risk: International travelers, institutions where prolong close
person to person contact occurs (army camps, institutions, schools,
day care centers), homosexuals.
Outcome
after infection with hepatitis A virus: Acute hepatitis A occurs
that almost always resolves. It never becomes smoldering disease
or chronic hepatitis. Rarely, in 0.3% cases it result in acute liver
failure requiring a liver transplant.
Common
manifestations of acute hepatitis A is loss of appetite, fatigue,
dark urine, nausea, headache, mild abdominal pain and low grade
self limiting fever. Jaundice (yellowness of eyes and skin) may
or may not occur. During acute stage of hepatitis patient's blood
and bodysecretions are infectious to others.
Diagnosis
is confirmed by special blood tests.
Vaccine
is available to prevent the occurrence of this disease.
ii.
Hepatitis B:
Infection
occurs by contaminated needle, contaminated body piercing and tattooing
equipments or sexual contact. Infants born to mothers with chronic
hepatitis get infected during child birth or early infancy in about
90% of the cases.
It
is estimated that word wide more there are more than 400 million
and in USA over 1.25 million chronic carriers of the disease. Globally
the disease accounts for 250,000 and in the USA 5,000 to 6,000 hepatitis
B related deaths each year.
Persons
at risk: Sexual transmission accounts for 1/3 of hepatitis B infection
in USA . Other risk groups include intravenous drug users, people
with hepatitis B infected person's household, residents of nursing
homes, hemodialysis and hemophilia patients, prison and prison workers.
Other persons at risk are healthcare workers, particularly those
exposed to accidental cuts and bruises and hemodialysis staff.
Outcome
after infection with hepatitis B virus: Acute hepatitis B occurs
following infection. Three things may happen thereafter:
Acute
hepatitis may slowly resolve with in six months without any chronic
disease. This happens in about 90-93% of acute hepatitis B in adults
and 50% of children with acute hepatitis B.
•
Chronic hepatitis B infection with continued smoldering liver injury
may result. This slowly progresses to scarring of liver and cirrhosis.
•
Carrier of hepatitis without progressive disease.
These
patients have no symptoms and usually do not have continued liver
injury. However, they may be still infective and pass infection
to others.
Acute
infection with hepatitis B virus manifests with is loss of appetite,
fatigue, dark urine, nausea, headache, mild abdominal pain and low
grade fever and Jaundice (yellowness of eyes and skin). At times,
acute hepatitis may not have any symptoms and go undetected. In
about 10% of cases this becomes chronic smoldering infection with
slow but continued liver injury leading to cirrhosis. It is estimated
that there are about 1.25 million chronic carriers of hepatitis
B in the USA . Risk of liver cancer is increased in patients with
chronic hepatitis B. Alcohol use increases the progress of liver
disease in hepatitis B
Diagnosis
is made by special blood tests.
Vaccine
is available that prevents the occurrence of the disease.
iii.
Hepatitis C:
This
hepatitis was called non-A non-B hepatitis. Infection commonly occurs
through sharing intravenous drug use paraphernalia, body piercing
or tattooing equipments or sexual contacts. Because of current screening
of blood donors, now a days blood transfusion is not a source of
hepatitis C infection.
The
hepatitis C virus, discovered in 1989, is transmitted via blood,
so anyone who had a blood transfusion before 1992 or has the above
mentioned predisposition is at risk of developing hepatitis C. It's
possible for an infected mother to pass along the virus to her child
at birth. Researchers aren't sure whether hepatitis C can be transmitted
sexually. If so, it's a rare occurrence, but people who've had multiple
partners are encouraged to be tested for the virus.
World
wide over 100 million and in the USA over 4 million people have
are infected with hepatitis C virus. It is the leading cause of
chronic liver disease. The hepatitis C virus kills between 10,000
and 12,000 Americans each year. The hepatitis C virus infection
is by far the leading indication for liver transplantation in the
United States, accounting for between 30% and 50% of liver transplants,
depending on the state where the patient lives
Persons
at risk: Blood transfusion prior to late 1992, intravenous drug
users, patients on hemodialysis and hemophilia patients, body piercing
and tattoo, military veterans who served in Vietnam, prisoners,
homeless and people with HIV.
Outcome
after infection with hepatitis C: Acute hepatitis C occurs following
infection. It becomes a smoldering disease with slow but progressive
injury or chronic hepatitis in 80-85% of cases. Chronic hepatitis
C progresses to cirrhosis over an extended period of 20-25 years
in about 25% patient.
Acute
infection with hepatitis C virus mostly remains undiagnosed because
patients usually do not have any symptoms. In about 1/3 of those
who do get symptoms they are mild and do not interfere with daily
activity. Patients may have loss of appetite, common- cold like
symptoms with fatigue, lethargy, body-ache, and headache. Usually
they do not have Jaundice (yellowness of eyes and skin).
Chronic
hepatitis C occurs in about 80-85% of those who have had acute infection
in the past. In most patients there are no symptoms and the diagnosis
is made at routine blood test when liver enzymes are incidentally
found to be increased leading to test for and detection of hepatitis
C virus. Usual symptoms are fatigue, dull pain in upper part of
abdomen on right side. In about 25% of patients with chronic hepatitis
C the disease progresses to cirrhosis in about 20-25 years. Risk
of liver cancer is increased in patients with chronic hepatitis
C. Alcohol use increases the liver disease in hepatitis C.
Diagnosis
is made by special blood tests.
No
vaccine is currently available for hepatitis C.
2.
Alcoholic Hepatitis:
Alcohol
can cause inflammation of liver (hepatitis). It occurs in both heavy
drinkers as well as in binge drinkers. This is described in subsequqent
pages under alcoholic liver disease.
3.
Autoimmune hepatitis: Autoimmune Hepatitis: Autoimmune Hepatitis:
This
is a condition wherein one's immune system starts attacking their
own organs, as if they did not belong to that individual. Autoimmune
hepatitis primarily affects women and starts as early as adolescence.
As the name suggests, autoimmune hepatitis can cause inflammation
of the liver and other symptoms common to liver disease such as jaundice
and itching as well as some associated with autoimmune disorders,
namely, aching joints. Fatigue, common to both, is a frequently reported
symptom. Lab tests show the presence of increased gamma globulin and
smooth muscle antibodies in the blood.
Many
people with autoimmune hepatitis respond well to prednisone treatment,
which can relieve symptoms and cause elevated liver enzyme levels
to return to normal. Autoimmune hepatitis is a condition that needs
monitoring over the long term, as it can lead to cirrhosis and ultimately,
the need for a liver transplant.
4.
Toxic hepatitis:
Rarely,
medications intended to help patients can cause the liver to become
inflamed causing toxic hepatitis. In an occupational setting, toxic
hepatitis can occur when workers are exposed to certain chemicals
in a confined space and are not wearing or properly using respiratory
protective gear. Other causes include certain medications, mushroom
poisoning etc.
Mushroom
poisoning : Eating wild mushrooms can make a person severely ill,
or in the worst-case scenario, cause a painful death. One particular
type of mushroom, the Amanita phalloides causes about 90 percent of
all mushroom eating-related deaths. Mushroom poisoning typically involves
a latent period of as long as 24 hours, when no symptoms are felt,
followed by extreme gastrointestinal upset; damage to several organs,
including the liver; heart failure; seizures; and coma.
The mushrooms' toxins can have an especially severe effect on the
liver, attacking the organ's cells and shutting down some of its key
functions. When the liver begins to fail but there is medical reason
to believe the patient could survive the poisoning, that person may
be a candidate for liver transplantation.
III. Obesity and Liver Disease; Non-alcoholic fatty liver disease (NAFLD) and Non-alcoholic steatohepatitis (NASH);
Consumption of alcohol is the most common cause of accumulation of excess fat in the liver. It is now recognized that similar fat accumulation in the little alcohol. This is known as non-alcoholic fatty liver disease (NAFLD). While in most of such cases the fatty liver is from obesity and the liver continues to function well and may not present a problem during their lifetime. However, in some obese patients excess fat causes inflammation in the liver known as Non-alcoholic steatohepatitis ( NASH). NASH, in some patients, may cause progressive liver injury resulting ultimately in cirrhosis and other complications of liver failure including liver cancer.
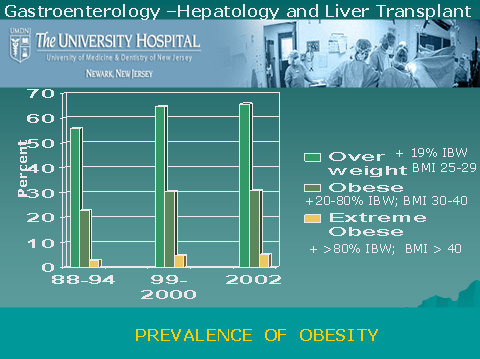
How Common Is Obesity Related Fatty Liver Disease:
Best estimates of prevalence of NAFLD are 18-20% and that of NASH is 4% in the general population. The prevalence of NASH increases with obesity and may rise to 40% in moderate to severely obese individuals. With the increasing incidence of obesity in the country NAFLD has become a growing problem. About two-third of adults are either overweight or obese, and about 9 million American children over age 6 are considered obese and same number are overweight.
Associated conditions:
NAFLD/NASH is associated with a metabolic complex characterized by diabetes mellitus, obesity, high blood pressure, high cholesterol/triglycerides (hyperlipidemia) and resistance to insulin.
Symptoms:
Most patients with NAFLD/NASH may not have any symptoms and in those that are symptomatic the manifestation are non-specific. Fatigue and occasional upper abdominal discomfort may be present in a small number of patients only. On examination liver may be enlarged in less than half of the patients. Most of the patients are between 40-60 years of age, but the disease is well described in children as well. Children are more prone to have symptoms of upper abdominal discomfort and pain as compared to the adults. In asymptomatic cases the finding of an abnormal liver chemistry (AST/ALT) at routine health check-up and absence of known cause of liver disease in an obese person is a strong indicator of the diagnosis of NAFLD/NASH.
Confirming the diagnosis of NAFLD/NASH:
Liver biopsy remains the gold standard but imaging of liver with ultrasound is a useful non invasive test.

Normal Liver cells without fat
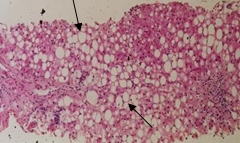
Fat deposits in Liver cells
Treatment of NAFLD/NASH involves modification of lifestyle, use of anti-oxidants, and avoidance of agents potentially toxic to the liver. Research is in progress to evaluate other medications that may selectively intervene at the mechanism that initiate the disease. A gradual weight reduction, abstinence from alcohol, better control of diabetes, and other concurrent illnesses are important to slow the progress of the disease. Patients should be followed closely for early detection of progressive liver injury or its complications including liver cancer.
IV. Acute Fulminant Hepatic Failure:
It is an acute catastrophic event with sudden onslaught of massive liver injury in a person who has had normal liver all along. The condition manifests with rapidly deteriorating liver function, progressive alteration in mental status leading to coma, deranged blood clotting and rapid onset of failure of kidneys, lungs and susceptibility to infection.
Causes of acute fulminant heptic Failure:
Majority of cases are due to virus infection or to drugs. Incidence of acute fulminant hepatitis in acute hepatitis A is less than 0.3%, in acute hepatitis B 1-4%, with hepatitis C it is very low. In one third of the cases no identifiable cause may be found. Amongst drugs Tylenol overdose is the most common cause. Other causes include liver failure in the last three months of pregnancy, a disease where abnormal amount of copper accumulates in liver (Wilson's disease) and mushroom poisoning. Urgent liver transplant is the only option in patient not showing signs of quick recovery.
V.
Alcoholic Liver Disease:
Heavy
drinking over a long period of time can take its toll on the liver.
Alcohol produces three types of liver injury:
a. Fatty liver: there is abnormal and excess accumulation of fat in liver
cells that interferes with its proper functioning.
b. Alcoholic hepatitis: Inflamed liver with liver injury.
c. Cirrhosis: Scarred liver with significant liver cell injury.
According
to the Scientific Registry of Transplant Recipients, alcoholic liver
disease was the third leading indication for liver transplantation in
2003 (26 percent of the transplant recipients in this category also
were infected with hepatitis C).
If alcoholic liver disease is identified in an early stage like fatty liver and if the person stops drinking, it is possible that his or her condition could improve. However, these are two major "ifs," considering the often-silent nature of liver disease and the difficulty of breaking an addiction. As the liver disease advances to cirrhosis these patients require liver transplant like any other patients with cirrhosis of liver.
Patients with alcoholic liver disease must meet the following criteria to be considered for liver transplantation at University Hospital:
a. abstinence from alcohol use
b. ongoing participation in an alcohol treatment program or support group
c. presence of an adequate psychosocial support system.
These
patients must enter a formal contract with the transplant team outlining
the parameters of abstinence from alcohol use.
VI.
Wilson's disease:
Normally,
the liver helps the body rid itself of copper. In people with Wilson's
disease, the gene responsible for this process is defective and copper
builds up in the liver, the brain, and other organs. Over time, too
much copper in the liver can lead to symptoms such as jaundice and swelling
of the abdomen and, untreated, lead to acute liver failure, a need for
liver transplantation, or death. Many patients, when diagnosed early
on, respond well to the drugs that help remove copper from the bloodstream.
They must take the medicine for the rest of their lives. There is an
acute form of Wilson's disease in which the copper overload is swift
and the organ damage is rapid . In patients with liver failure
from wilson's disease liver transplantation is life saving.
VII.
Hemochromatosis:
It
is a disease of excess iron deposition in the liver and other organs
of the body. Excess iron deposits in the liver damages the liver with
destruction of liver cells and accumulation of scar leading to cirrhosis
(scarred liver) that can not function. Hemochromatosis affects one in
every 300 to 400 people. It is genetically inherited disease. The prevalence
of the gene for hemochromatosis is not uncommon (10%) in people of North-Western
European descent. To be affected by the disease person has to have acquired
the gene from each of the parents. Family history and follow-up of immediate
relatives of patients with hemochromatosis is important.
Symptoms
usually develop between the ages of 40-60 years of age. Liver damage
usually causes jaundice (yellowing of eyes and skin). Excess iron deposition
in other organs may manifest as joint pain (arthritis), Diabetes (pancreas
damage) skin pigmentation, heart abnormality (deposit of iron in heart),
and hormonal problems (iron in pituitary gland).
Diagnosis
is made by special blood tests to look for iron parameters, genetic
markers, and measurement of iron from ma sample of liver tissue obtained
by doing liver biopsy.
As
the disease progresses to advances scarring (cirrhosis) other features
of liver failure namely fluid accumulation, altered mental state, coagulation
problems appear. Liver transplant is the only treatment option with
progressive disease
Other
Liver Diseases:
Alpha
1-Antitrypsin (AAT) Deficiency.
AAT
(also known as alpha1 proteinase inhibitor) is a protein that is made
primarily in the liver. This belongs to a group of proteins, which
help prevent certain white blood cell enzymes (proteinases) from
going beyond their regular infection-fighting functions to attack
healthy body tissue. When the body doesn't make enough AAT, the lungs
often don't work as efficiently (patients tend to develop emphysema)
and the liver may be adversely affected, leading to cirrhosis. AAT
deficiency is an inherited, condition, with two defective genes passed
along�one by each parent. This rare deficiency affects fewer than
100,000 Americans.
Familial
Amyloidosis Polyneuropathy.
This
inherited disease, which occurs most often in people of Swedish and
Portuguese descent, is a mutation of the transthyretin (TTR) molecule.
Instead of the TTR protein being formed, an incorrect protein, amyloid,
is produced. With this condition, amyloids are found throughout the
body, destroying nerves and interfering with other organs. Neurological
symptoms, low blood pressure, and muscle wasting are common manifestations
of the disease, which can run a course of several years but has no
cure. Because TTR is made in the liver, liver transplantation has
been used as treatment.